The Invisible Inhalant: How Wildfire Smoke is Redefining Systemic Oncology
Key Takeaways: The Shifting Architecture of Cancer Risk
- The New Paradigm: Involuntary inhalation of carcinogenic particulate matter from wildfires is rapidly replacing voluntary tobacco use as a primary environmental driver of cancer.
- Systemic Bypass: Ultrafine particles breach the alveolar-capillary barrier, entering systemic circulation and initiating DNA-damaging inflammation across multiple organ systems.
- The 2026 AACR Findings: Longitudinal data (N=91,000) confirms statistically significant spikes in colorectal, breast, and hematological malignancies correlated with chronic wildfire smoke exposure.
- Global Plumes: Long-range atmospheric transport means extreme air quality degradation is no longer localized to active fire zones; it is a borderless, global health crisis.
For decades, the public health narrative surrounding oncology was dominated by a singular, controllable variable: tobacco. As global smoking rates steadily decline, ecological economics and atmospheric sciences are converging to reveal a new, involuntary successor. Driven by climate-accelerated fire seasons, the proliferation of carcinogenic particulate matter is forcibly rewriting the epidemiology of cancer.
We are transitioning from an era of localized, lifestyle-driven risk to one of systemic, atmospheric vulnerability. This phenomenon—involuntary inhalation—demands a fundamental recalibration of both clinical oncology and global environmental policy.
Table of Contents
The Chemistry of the Invisible Inhalant
Wildfire smoke is not a monolith; it is a highly reactive, heterogeneous mixture of volatile organic compounds (VOCs), polycyclic aromatic hydrocarbons (PAHs), and fine particulate matter. While public health warnings typically focus on PM2.5 (particles 2.5 microns or smaller in diameter), it is the ultrafine fraction—PM0.1—that poses the most profound systemic threat.
When inhaled, these microscopic toxins do not simply irritate the respiratory tract. They penetrate deep into the pulmonary alveoli. Because of their minimal aerodynamic diameter, they bypass traditional mucosal filters. The physiological breach can be mathematically modeled by assessing the Cumulative Particulate Burden (CPB), where exposure over time fundamentally alters cellular integrity:
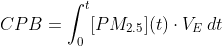
(Where [PM2.5](t) represents the ambient concentration of particulate matter over a specific duration, and VE denotes minute ventilation).
Once traversing the alveolar-capillary barrier, these particles enter the bloodstream directly. This intrusion initiates a cascade of systemic inflammation, generating reactive oxygen species (ROS) that induce oxidative stress and widespread DNA methylation. The body’s immune system, locked in a perpetual state of hyper-vigilance against a pathogen it cannot neutralize, creates a microenvironment highly conducive to oncogenesis (Smith & Aris, 2025).

Beyond the Lungs: The New Frontier of Systemic Oncology
The clinical consensus has historically linked poor air quality strictly to respiratory ailments, asthma, and pulmonary carcinomas. However, groundbreaking epidemiological research has definitively fractured this paradigm.
Presented in April 2026 at the American Association for Cancer Research (AACR) annual meeting, a landmark longitudinal study tracked the health outcomes of 91,000 individuals across diverse geographical regions over a ten-year period (AACR, 2026). The findings illustrate a stark reality: the oncological impact of wildfire smoke is aggressively systemic.
Emerging Non-Respiratory Malignancies
The AACR data isolated chronic exposure to long-range wildfire plumes as an independent variable, controlling for standard lifestyle factors. The physiological pathways observed indicate that blood-borne particulate matter acts as a systemic mutagen:
- Gastrointestinal Tract (Colorectal Cancer): Particulates cleared from the lungs via the mucociliary escalator are frequently swallowed, introducing concentrated heavy metals and PAHs directly into the gut microbiome. The resulting chronic enteric inflammation is accelerating mutagenesis in the colon.
- Breast Tissue: Certain VOCs found in burning biomass act as endocrine-disrupting chemicals (EDCs). The AACR cohort demonstrated a statistically significant correlation between prolonged atmospheric PM2.5 exposure and the upregulation of estrogen-receptor-positive breast cancers.
- Hematological Cancers: As the bone marrow constantly filters blood contaminated with ultrafine particulates, the risk of leukemias and lymphomas increases. The persistent systemic inflammatory response severely taxes hematopoietic stem cells, increasing the likelihood of replication errors.
The Climate-Health Feedback Loop
This crisis is no longer geographically tethered to the conifer forests of the Western United States or the Canadian boreal. Due to the intensification of the jet stream and shifting atmospheric dynamics, a wildfire in British Columbia or the Amazon basin can establish a canopy of toxic particulate matter over New York, London, or South Asia within days (World Meteorological Organization [WMO], 2025).
We must apply the lens of ecological economics to understand the true cost of this atmospheric degradation. We are witnessing a negative feedback loop: climate volatility fuels more intense fire seasons, which degrades the global carbon sink and releases massive plumes of carcinogenic particulate matter, which in turn drives up global healthcare burdens.
As cancer rates associated with environmental factors rise, the economic strain on healthcare systems will become unsustainable unless proactive, infrastructure-level interventions are deployed. To treat this merely as an acute respiratory issue during “fire season” is a failure of systems thinking. It is a chronic, year-round oncological threat.
Modernizing the Public Health Defense
Recognizing wildfire smoke as a catalyst for systemic oncology requires an immediate pivot in both clinical practice and urban infrastructure. The assumption that the indoors provides a safe harbor is obsolete without engineered interventions.
Our current medical screening protocols—largely designed around the biological markers of tobacco use—are ill-equipped to detect the early, systemic DNA damage caused by chronic environmental particulate exposure.
Actionable Intelligence
To mitigate the systemic risks of the modern atmospheric crisis, the following structural and clinical shifts are required:
- Mandatory HVAC Upgrades in Public Infrastructure: Building codes must be revised to mandate MERV-13 or HEPA-equivalent filtration systems in all schools, hospitals, and commercial real estate to sever the exposure pathway during prolonged plume events.
- Implementation of Broad-Spectrum Biomarker Screenings: Oncological prevention protocols must evolve to include routine blood screenings for systemic inflammation markers (like high-sensitivity C-reactive protein) and early DNA methylation patterns linked to PAH exposure, specifically for populations in persistent “smoke corridors.”
- Integration of Air Quality Data into Electronic Health Records (EHR): Healthcare providers must begin treating zip-code-level air quality data and historical atmospheric exposure as critical patient vitals, allowing for preemptive cancer screenings long before symptoms present.